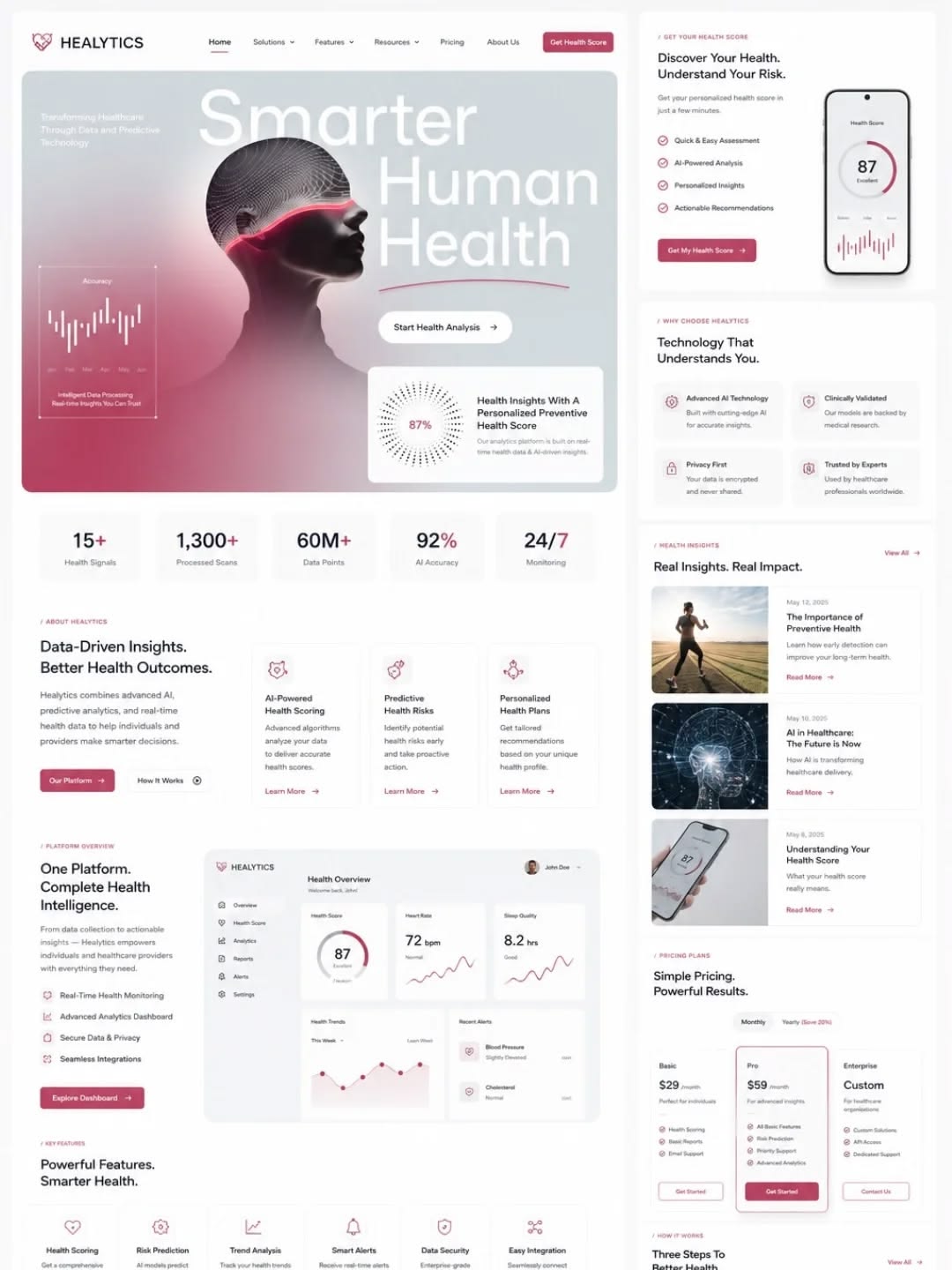
Understand risk
Screening models read structured answers, not guesses.
Self-assessments use form responses, age, vitals, history, and risk factors to return a clear risk band and next-step guidance.
Health AI
Moesha and the AfyaRekod model layer organize risk screening, symptom extraction, vitals analysis, imaging workflows, and governed recommendations with clear safety boundaries.
Understanding the system
Each workflow is separated by what the patient is doing, how quickly the answer is needed, and how much clinical governance is required before an output appears.
Self-assessments use form responses, age, vitals, history, and risk factors to return a clear risk band and next-step guidance.

The symptom extractor identifies medical keywords, body areas, duration, severity, and red flags from patient notes and imported records.
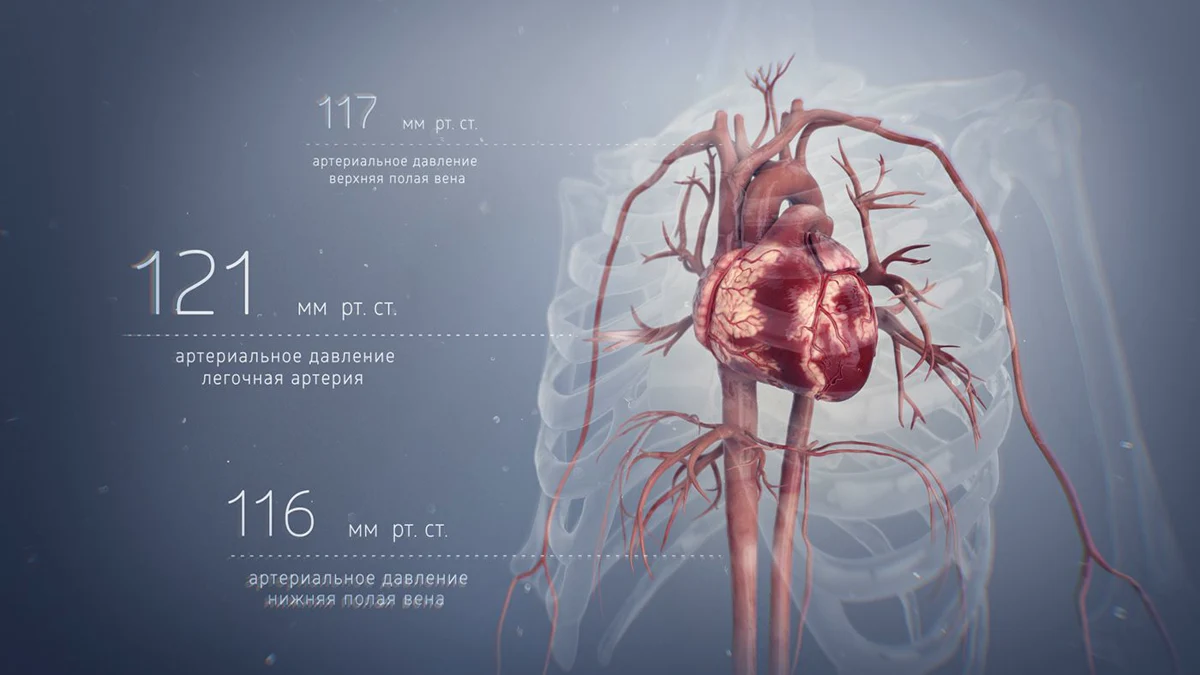
Pulse, blood pressure, temperature, SpO2, glucose, and diary patterns can be reviewed for trend shifts and escalation thresholds.
Camera, wound, skin, scan, and radiology workflows can be queued for heavier review where auditability matters more than speed.
Patient experience
The AI layer should make the record easier to act on. A patient can ask about symptoms, review a result, prepare for a visit, or understand when a clinician should be involved.
See dashboard flow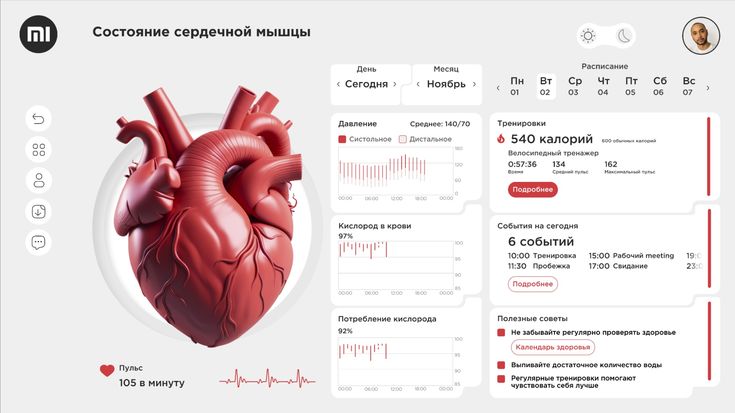
Capability groups
The page separates patient-facing support from heavier clinical workflows so the product feels useful, explainable, and careful.
Structured risk screening for diabetes, hypertension, stroke, cancer, and TSC depression survey workflows.
Patient-facingCT, MRI, X-ray, and ultrasound analysis should run asynchronously because imaging is heavier and GPU-expensive.
Clinician-assistedDiagnosis, prognosis, vitals analysis, and recommendations are routed through governed clinical endpoints.
Care pathway supportExtract symptoms, diseases, and body-part context from patient text and imported clinical records.
Records and symptom flows
Moesha explains records, prepares questions, and guides next actions without replacing a qualified clinician.
Patient guidance
Real-time vs async
This keeps the patient experience responsive while reserving heavier compute for imaging, segmentation, coding, and batch analytics.
The user is waiting in the app after submitting a form.
Managed CPU endpoint or lightweight inference serviceNeeded during the symptom flow and later for record normalization.
Guardrailed LLM/RAG service with clinical retrievalClinician and patient workflows need low-latency but governed output.
Governed inference endpoint, stream processor, and online feature storeImages are heavier, GPU-expensive, and rarely require sub-second output.
Async GPU inference or scheduled batch processingSurvey-based risk screening should run after form submission, not continuous monitoring.
CPU endpoint or background workerGovernance
Model cards, interpretability, fairness review, and validation gates keep Health AI trustworthy and auditable.
Every model needs signed clinical review before it is promoted to production use.
SHAP, LIME, attention maps, or equivalent explanations must be available for governed outputs.
Input distribution, prediction drift, and embedding drift are monitored before retraining is triggered.
Patient-facing AI explains and guides; it does not diagnose or replace a qualified clinician.
Health AI should explain, prepare, summarize, and escalate. It should stay grounded in records, guidelines, consent, and clinical governance.
Open prototype